ENFERMERÍA CUIDÁNDOTE - ISSN 2695-9364
Camarero Gómez MP, Munuera Martínez PV, Páez Moguer J. Thermal analysis of the diabetic foot using mobile infrared thermography: A pilot study in primary care
Thermal analysis of the diabetic foot using mobile infrared thermography: A pilot study in primary care
Análisis térmico del pie diabético mediante termografía infrarroja móvil: Estudio piloto en atención primaria
Authors:
- María Pilar Camarero Gómez
 . Malaga-Guadalhorce Health District. Malaga. Spain.
. Malaga-Guadalhorce Health District. Malaga. Spain. - Pedro Vicente Munuera Martínez. Faculty of Nursing, Physical Therapy, and Podiatry. University of Seville. Seville. Spain.
- Joaquín Páez Moguer. Faculty of Health Sciences. University of Malaga. Malaga. Spain.
- María Pilar Camarero Gómez. Malaga-Guadalhorce Health District. Malaga. Spain.
E-mail: pcamarerog@gmail.com
- 20/04/2025
- 14/07/2025
- 28/05/2026
- Camarero Gómez MP, Munuera Martínez PV, Páez Moguer J. Thermal analysis of the diabetic foot using mobile infrared thermography: A pilot study in primary care. Enferm Cuid. 2026;9. https://doi.org/10.51326/ec.9.9130415
 Las obras se publican en esta revista bajo una licencia Creative Commons Attribution 4.0 International License (CC BY 4.0) que permite a terceros utilizar lo publicado siempre que mencionen la autoría del trabajo y a la primera publicación en esta revista.
Las obras se publican en esta revista bajo una licencia Creative Commons Attribution 4.0 International License (CC BY 4.0) que permite a terceros utilizar lo publicado siempre que mencionen la autoría del trabajo y a la primera publicación en esta revista.
|
Abstract Introduction: Infrared thermography is a non-invasive tool for early detection of complications associated with the diabetic foot. Objective: To evaluate the usefulness of mobile infrared thermography as a complementary screening technique for diabetic patients in primary care settings. Methods: A cross-sectional observational study with 20 diabetic patients was conducted at a primary care center in Málaga, Spain. Thermal images were captured following the TISEM consensus using a FLIR One Edge Pro® device. Thermographic variables including the Thermal Risk Index and thermal asymmetry were analyzed with ThermoHuman® software and correlated with clinical variables such as neuropathy, ankle–brachial index, and self-care knowledge. Results: Forty-five percent of participants showed moderate to high risk of ulceration according to the International Working Group on the Diabetic Foot. No significant differences in thermal asymmetry were found over time (p > 0.05). Mixed-effects modelling did not reveal significant associations between ankle–brachial index, neuropathy, and thermal asymmetry. Conclusions: Mobile infrared thermography can detect plantar thermal changes related to ulceration risk. However, further studies are needed to support its systematic implementation in diabetic foot screening. Keywords: Diabetic Foot; Diabetic Neuropathies; Early Diagnosis; Infrared Thermography; Peripheral Arterial Disease; Primary Health Care. |
|
Resumen Introducción: La termografía infrarroja (TI) se postula como una herramienta no invasiva y objetiva para la detección precoz de complicaciones en el pie diabético. Objetivos. Evaluar la utilidad de la TI móvil como técnica de cribado complementaria en personas con diabetes mellitus en un entorno de atención primaria. Metodología: Estudio observacional, descriptivo y transversal realizado con 20 pacientes diabéticos en un centro de salud de Málaga. Se aplicó un protocolo basado en el consenso TISEM para la captura de imágenes con cámara FLIR One Edge Pro®. Se analizaron variables termográficas como el índice de riesgo térmico (TRI) y la asimetría térmica mediante software ThermoHuman®. Se correlacionaron con variables clínicas como neuropatía, ITB, y conocimientos de autocuidados. Resultados: El 45% de los sujetos presentó riesgo moderado-alto de ulceración según IWGDF. No se observaron cambios significativos en la asimetría térmica a lo largo del tiempo (p > 0.05). El modelo de efectos mixtos no encontró asociaciones significativas entre ITB, neuropatía y asimetría. Conclusiones: La termografía infrarroja móvil permite detectar alteraciones térmicas plantares relacionadas con factores de riesgo para ulceración, aunque son necesarias más investigaciones para establecer su aplicabilidad sistemática en el cribado. Palabras clave: Diagnóstico Precoz; Enfermedad Arterial Periférica; Neuropatías Diabéticas; Pie Diabético; Prevención Primaria; Termografía Infrarroja. |
|
Introduction Diabetes mellitus is one of the most prevalent chronic diseases of the 21st century, and its impact on public health continues to grow. The 11th edition of the IDF Diabetes Atlas estimates that, in 2024, approximately 643 million adults (aged 20–79 years) are living with diabetes, with projections exceeding 850 million by 2050, driven by rising obesity rates, physical inactivity, and unhealthy dietary patterns1,2. The global prevalence among adults is currently 10.9% and is expected to increase to 11.8% over the next 25 years, with the greatest increases anticipated in low- and middle-income countries2. One of the most severe and costly complications of diabetes is diabetic foot, characterized by ulceration, infection, or destruction of foot tissues associated with neuropathy and/or peripheral arterial disease3. These lesions are associated with high rates of morbidity, hospitalization, amputations, and mortality. It is estimated that up to 85% of diabetes-related amputations are preceded by a foot ulcer4, with an average hospital cost per episode exceeding €7,000 in Spain5. In Andalusia, lower-limb amputation rates remain high. In 2019, 2.7 amputations per 1,000 individuals with diabetes were reported, a figure that temporarily decreased in 2020, likely due to the confinement measures during the COVID-19 pandemic6. The International Working Group on the Diabetic Foot (IWGDF) defines diabetic foot as infection, ulceration, or destruction of foot tissues associated with neuropathy and/or peripheral arterial disease in individuals with diabetes mellitus3,7. Foot ulcers represent one of the most serious complications of diabetes, with a significant impact on quality of life, healthcare burden, and economic costs. They are also associated with an increased risk of cardiovascular events and mortality8,9. Up to 70% of patients with diabetic foot may eventually undergo amputation, and 85% of cases are preceded by an ulcer that progresses to gangrene or severe infection3,10. Risk factors for amputation include clinical variables such as neuropathy and vascular disease, as well as social and demographic determinants3. The five-year survival rate after the onset of a diabetic foot ulcer is approximately 50–60% and decreases further when major amputation is required3,4,11. Early diagnosis is therefore essential to prevent severe complications. Prevention programs should focus on the early identification of warning signs and the implementation of effective screening strategies12. In this context, infrared thermography has emerged as a promising technique enabling the detection of cutaneous thermal alterations associated with inflammation, ischemia, or neuropathy. Its application through mobile devices may facilitate its use in primary care settings and in environments with high clinical workload8,13. This non-invasive and objective tool allows for the quantification of temperature differences associated with early tissue damage, prior to the appearance of visible lesions8. Consequently, infrared thermography represents a technology with potential to be integrated into diabetic foot screening protocols. However, its clinical applicability, diagnostic reliability, and relationship with established risk factors require further validation in prospective studies. Accordingly, the aim of the present study was to evaluate the effectiveness of infrared thermography as a complementary tool to identify patients with diabetes mellitus at risk of developing foot complications, such as neuropathic ulcers and peripheral arterial disease (Figure 1).  Figure 1. Bilateral plantar thermographic image showing temperature distribution patterns. Areas of increased temperature (red) and decreased temperature (blue/green) reflect variations in plantar thermal response, potentially associated with underlying inflammatory, vascular, or biomechanical factors. Methodology A descriptive, observational, and cross-sectional study was conducted in a primary care setting within the Andalusian Public Health System (Huelin Health Center, Málaga, Spain). The selection of thermographic variables and their analysis were based on the available scientific evidence on infrared thermography in diabetic foot, gathered through a narrative review of the literature. The search was performed in PubMed/MEDLINE, Scopus, Web of Science, Cochrane Library, and CINAHL databases, prioritizing publications from 2014 to 2024 in English and Spanish. Controlled vocabulary (DeCS/MeSH) terms such as Infrared Thermography, Diabetic Foot, Peripheral Arterial Disease, Diabetic Neuropathies, Primary Health Care, and Screening were used to guide the theoretical and technical framework of the study. The study was approved by the Research Ethics Committee of the Andalusian Regional Government (CEIm Provincial de Málaga), as stated in the favorable report issued during session no. 12 on December 19, 2024 (approval code: SICEIA-2024-001888). The project, entitled Applicability of Mobile Infrared Thermography in the Evaluation of the Diabetic Foot (TERMOPIE), was conducted in accordance with current regulations on biomedical research, medicinal products, and personal data protection (Law 14/2007, Royal Legislative Decree 1/2015, and Organic Law 3/2018). Participants The sample consisted of 20 patients with type 1 and type 2 diabetes mellitus, selected through consecutive sampling from individuals enrolled in a diabetic foot screening program. Inclusion criteria:
Exclusion criteria:
Collected Variables Sociodemographic and clinical variables were recorded, including age, body mass index, glycated hemoglobin (HbA1c), duration of diabetes, level of physical activity, smoking status, and the presence of hypertension, retinopathy, foot deformities, and joint limitations. Functional variables were also assessed, including pedal and posterior tibial pulses, ankle–brachial index(ABI), and peripheral neuropathy evaluated using the 10 g monofilament (Figure 2) and 128 Hz tuning fork (Figure 3). Ankle–brachial index (ABI) was measured using a handheld Doppler device and sphygmomanometer (Figure 4). Additionally, self-care level was assessed using the DSFQ-UMA questionnaire. Environmental conditions (room temperature and humidity) were recorded, and patients were stratified according to risk using the IWGDF and SAS classification systems.  Figure 2. Assessment of superficial sensation using a 10 g monofilament.  Figure 3. Evaluation of vibratory sensation using a 128 Hz tuning fork.  Figure 4. Measurement of the ankle–brachial index using a handheld Doppler device and sphygmomanometer. Instrumentation and Procedure Thermal images were acquired using a FLIR ONE Edge Pro® thermal camera (Figure 5) connected via Bluetooth to a smartphone, with a thermal resolution of 160 × 120 pixels and a thermal sensitivity of 70 mK.  Figure 5. FLIR ONE Edge Pro® thermal camera The procedure was standardized according to the TISEM (Thermographic Imaging in Sports and Exercise Medicine) consensus (Figure 6), which establishes the following conditions:
 Figure 6. Standardized positioning with a cold black background and the camera placed perpendicular to the plantar surface of the foot, according to the TISEM protocol.  Figure 7. Plantar thermographic image acquired using a FLIR ONE Edge Pro® camera. During the examination, patients remained in a supine position, without socks or footwear. A total of five thermographic images were obtained for each participant. A representative example is shown in Figure 7.
A black cardboard support with plantar openings was used to standardize thermal contrast, and the camera emissivity was set at 0.98, corresponding to the emissivity value of human skin. Image Analysis The thermographic images were processed using ThermoHuman® software (Figure 8), which automatically segments the plantar regions of the foot and allows extraction of the following variables:
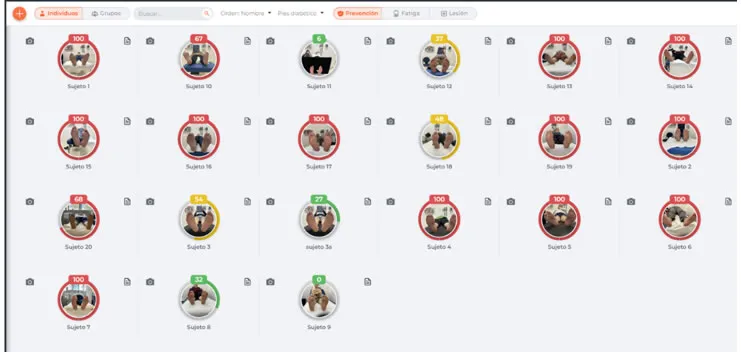 Figure 8. Thermal Risk Index (TRI) of the study participants obtained using ThermoHuman® software. Data Analysis Statistical analysis was performed using R software (version 4.4.0, April 24, 2024) and RStudio (version 2024.04.1 +748). Three different datasets were used:
Descriptive analyses and longitudinal analyses using mixed-effects models were conducted to assess the temporal evolution of thermographic variables and their association with clinical variables such as ABI, presence of neuropathy, HbA1c, and level of self-care. Ethical Considerations The study was conducted in accordance with the principles of the Declaration of Helsinki, and written informed consent was obtained from all participants prior to participation. Data were anonymized and handled in compliance with current data protection regulations, including Regulation (EU) 2016/679. Results Data from 20 patients with diabetes mellitus were analyzed, describing their clinical and demographic characteristics, as well as thermographic variables obtained at five measurement time points. The mean age of participants was approximately 65 years, and the mean body mass index was within the obesity range (32.37 kg/m²). The average glycated hemoglobin (HbA1c) was 7.50%, indicating moderate glycemic control. The mean duration of diabetes was 13 years, reflecting a population with long-standing disease. Regarding lifestyle habits, 80% of participants were non-smokers, and 60% reported engaging in some form of physical activity, although only 25% performed moderate-intensity exercise. Hypertension was present in 70% of participants, and a similar proportion exhibited foot deformities. Ankle joint limitation was highly prevalent. Retinopathy was observed in 45% of participants, while chronic kidney disease was present in only 5%. Most participants retained adequate sensory perception according to monofilament and tuning fork testing, although signs of neuropathy were identified in approximately one-third of the sample. According to IWGDF risk stratification, 45% of patients were classified as moderate risk, 30% as very low risk, 15% as low risk, and 10% as high risk. In contrast, application of the Andalusian Diabetic Foot Screening Protocol resulted in a markedly different distribution: 75% of participants were classified as high risk and 25% as moderate risk, with no individuals identified in the low or very low risk categories. Regarding thermographic variables, five measurements per participant were obtained, resulting in a total of 100 observations. Bilateral plantar thermographic image showing temperature distribution patterns is presented in Figure 1. The variables analyzed were TRI and mean thermal asymmetry (ASYMMETRY). TRI showed a high concentration of maximum values, limiting its discriminative capacity. The distribution of the Thermal Risk Index (TRI) across participants is shown in Figure 8. In contrast, ASYMMETRY presented a more balanced distribution closer to normality and was therefore selected as the dependent variable for longitudinal analyses. The analysis of ASYMMETRY over time, across five measurement points (pre-exercise, immediately post-exercise, and at 5, 10, and 15 minutes post-exercise), did not show statistically significant differences according to repeated-measures ANOVA (p = 0.336). This result remained unchanged after sphericity correction (Greenhouse–Geisser), thus no post hoc analyses were required. To further explore potential associations between ASYMMETRY and relevant clinical variables, a mixed-effects model was constructed including time, presence of neuropathy, and right and left ABI as fixed effects. This model also did not yield statistically significant associations, indicating that neuropathy, time points, and ABI values did not significantly influence plantar thermal asymmetry. However, residual inter-individual variance was high (0.811), suggesting considerable variability between participants. Discussion Early detection of underlying conditions that compromise the integrity of foot skin and tissues prior to the appearance of visible lesions, currently represents a priority in diabetic foot research. Timely diagnosis is essential to prevent adverse outcomes such as ulcers and amputations. In this context, infrared thermography has shown potential as a non-invasive technique capable of identifying subtle thermal changes associated with inflammatory, neuropathic, or ischemic processes on the plantar surface12. One of the most widely studied indicators is localized temperature increase, which may precede ulcer development. In routine clinical practice, thermal assessment is typically performed by manual palpation, a subjective method with limited sensitivity and poor reproducibility for detecting small temperature differences. In contrast, thermography enables objective, real-time, and contactless measurement of skin temperature distribution, potentially improving diagnostic capacity, particularly in primary care settings15,16. Despite these advantages, several challenges remain for the systematic implementation of infrared thermography in clinical practice. These include limited robust clinical evidence, the lack of consensus on the interpretation of thermal patterns, and the absence of standardized thresholds or priority anatomical regions. For instance, segmentation based on angiosomes—such as those defined by Taylor and Palmer (medial plantar artery, lateral plantar artery, medial calcaneal artery, and lateral calcaneal artery)—has been proposed as an anatomically coherent approach, although its application is not yet standardized8,13,17. Furthermore, not all thermal asymmetries indicate tissue damage, and not all lesions present with evident thermal imbalance. Therefore, thermography should be considered a complementary tool that provides useful physiological information but requires integration with other clinical and diagnostic methods18 Regarding equipment, devices with a standard resolution of 320 × 240 pixels and thermal sensitivity ≤0.1 °C are most commonly used in clinical research. However, advances in portable technologies have promoted the use of smartphone-based thermal cameras, such as the FLIR ONE Edge Pro® (160 × 120 pixels). Although these devices have lower resolution, they have demonstrated acceptable validity for preliminary screening, particularly in high-demand clinical settings (19,20). Kanazawa et al. reported that these devices allow rapid and efficient image acquisition, supporting their use in diabetic foot monitoring21. With respect to thermogram analysis, visual interpretation may be subject to bias, particularly in the absence of specific training. In this regard, computer-aided diagnosis (CAD) systems represent a promising advancement. These systems enable automated segmentation, quantification of variables such as mean thermal asymmetry, and objective classification of ulceration risk, thereby reducing inter-observer variability and improving reproducibility22. Recent studies have also highlighted the potential clinical and economic benefits of the systematic use of TRI as a screening tool. Models applied to the Finnish healthcare system estimate that routine TRI use could prevent severe complications and generate annual savings of up to €1.7 million14. In our study, risk stratification according to IWGDF criteria revealed a substantial proportion of patients at moderate and high risk, reinforcing the importance of identifying complementary tools for early assessment. Notably, discrepancies were observed between the stratification systems used. While the IWGDF classified 45% of patients as moderate risk, 30% as very low risk, 15% as low risk, and 10% as high risk, the Andalusian protocol classified 75% as high risk and 25% as moderate risk, with no patients in lower-risk categories. These differences may be explained by the distinct criteria considered: the IWGDF prioritizes loss of protective sensation, deformities, and ulcer history, whereas the Andalusian protocol incorporates additional clinical variables such as hypertension, retinopathy, and self-care practices (e.g., smoking or inappropriate nail care). This methodological divergence highlights the need to harmonize criteria and adapt risk stratification systems to the clinical context in which they are applied. The high residual variance (0.811) observed in the mixed-effects model indicates substantial inter-individual variability, possibly related to factors not captured in the analyzed variables, such as microcirculatory status or treatment adherence. This finding underscores the complexity of diabetic foot assessment when approached from a single diagnostic perspective. Strengths and Limitations This pilot study presents several strengths including the standardized application of the TISEM protocol, the use of portable thermographic technology in a primary care setting, the integration of clinical and thermographic variables, and the use of automated analysis software. Nevertheless, several limitations should be acknowledged, including the small sample size (n = 20), limiting generalizability, the absence of a control group (patients without diabetes or without clinical risk), the use of a single geographic setting, reducing population representativeness, and the limited resolution of the thermal device, which may affect measurement accuracy. Despite these limitations, this study demonstrates the feasibility of implementing a rigorous thermographic assessment protocol for diabetic foot in a real-world primary care setting. The reproducibility of the measurements, the high level of patient acceptability, and the integration with clinical variables provide a solid foundation for future research. Conclusion Infrared thermography represents a promising tool in the assessment of the diabetic foot, though its widespread implementation requires overcoming methodological, technological, and training-related challenges. In this pilot study, the use of mobile infrared thermography allowed the characterization of plantar thermal profiles in patients with diabetes mellitus, demonstrating its feasibility as a complementary tool in primary care settings. However, no statistically significant associations were observed between thermal asymmetry and clinical variables such as neuropathy or the ABI. This finding may be attributed to the small sample size and the high inter-individual variability not explained by the variables collected. Future research involving standardized protocols, multicenter clinical validation, and larger longitudinal studies is needed to establish more robust and clinically meaningful relationships between thermographic findings and diabetic foot risk factors. This evidence will be essential to support integration of infrared thermography into comprehensive strategies for the prevention and monitoring of diabetic foot complications.
References |
|
1. GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402(10397):203-34. https://doi.org/10.1016/s0140-6736(23)01301-6 2. International Diabetes Federation. IDF Diabetes Atlas. 11th ed. [Brussels]: International Diabetes Federation; 2025. Available from: https://diabetesatlas.org/resources/idf-diabetes-atlas-2025/ [Consultado 01-06-2025] 3. Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic Foot Ulcers: A Review. JAMA. 2023;330(1):62-75. https://doi.org/10.1001/jama.2023.10578 4. Armstrong DG, Boulton AJM, Bus SA. Diabetic Foot Ulcers and Their Recurrence. N Engl J Med. 2017;376(24):2367-75. https://doi.org/10.1056/nejmra1615439 5. Nieto-Gil P, Ortega-Avila AB, Pardo-Rios M, Cobo-Najar M, Blasco-Garcia C, Gijon-Nogueron G. Hospitalisation Cost of Patients with Diabetic Foot Ulcers in Valencia (Spain) in the Period 2009⁻2013: A Retrospective Descriptive Analysis. Int J Environ Res Public Health. 2018;15(9):1831. https://doi.org/10.3390/ijerph15091831 6. Aguilar Diosdado M, Almaraz Almaraz MC, Castro Campos JL, Contreras Rubio JR, Doiz Artazcoz E, Forcada Falcón M, et al. Pie diabético: documento de apoyo. [Sevilla]: Consejería de Salud y Consumo; 2023. Available from: https://www.juntadeandalucia.es/sites/default/files/inline-files/2023/12/DA_PieDiabetico_FINAL.pdf [Accessed 2024 May 01] 7. Bus SA, Sacco ICN, Monteiro-Soares M, Raspovic A, Paton J, Rasmussen A, et al. Guidelines on the prevention of foot ulcers in persons with diabetes (IWGDF 2023 update). Diabetes Metab Res Rev. 2024;40(3):e3651. https://doi.org/10.1002/dmrr.3651 8. Faus Camarena M, Izquierdo-Renau M, Julian-Rochina I, Arrébola M, Miralles M. Update on the Use of Infrared Thermography in the Early Detection of Diabetic Foot Complications: A Bibliographic Review. Sensors (Basel). 2023 Dec 31;24(1):252. https://doi.org/10.3390/s24010252 9. Stedman M, Robinson A, Dunn G, Meza-Torres B, Gibson JM, Reeves ND, et al. Diabetes foot complications and standardized mortality rate in type 2 diabetes. Diabetes Obes Metab. 2023;25(12):3662-70. https://doi.org/10.1111/dom.15260 10. Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis. Ann Med. 2017;49(2):106-16. https://doi.org/10.1080/07853890.2016.1231932 11. Godavarty A, Leiva K, Amadi N, Klonoff DC, Armstrong DG. Diabetic Foot Ulcer Imaging: An Overview and Future Directions. J Diabetes Sci Technol. 2023;17(6):1662-75. https://doi.org/10.1177/19322968231187660 12. Hernandez-Guedes A, Arteaga-Marrero N, Villa E, Callico GM, Ruiz-Alzola J. Feature Ranking by Variational Dropout for Classification Using Thermograms from Diabetic Foot Ulcers. Sensors (Basel). 2023;23(2):757. https://doi.org/10.3390/s23020757 13. Evangeline NC, Srinivasan S. Application of Infrared Thermography in Assessment of Diabetic Foot Anomalies: A Treatise. En: Borah MD, Laiphrakpam DS, Auluck N, Balas VE, editores. Big Data, Machine Learning, and Applications. Proceedings of the 2nd International Conference, BigDML 2021. LNEE, vol 1053. Singapore: Springer; 2024. p. 555-67. https://doi.org/10.1007/978-981-99-3481-2_43 14. Kurkela O, Lahtela J, Arffman M, Forma L. Infrared Thermography Compared to Standard Care in the Prevention and Care of Diabetic Foot: A Cost Analysis Utilizing Real-World Data and an Expert Panel. Clinicoecon Outcomes Res. 2023;15:111-23. https://doi.org/10.2147/ceor.s396137 15. Gatt A, Formosa C, Cassar K, Camilleri KP, De Raffaele C, Mizzi A, et al. Thermographic patterns of the upper and lower limbs: baseline data. Int J Vasc Med. 2015;2015:831369. https://doi.org/10.1155/2015/831369 16. Gatt A, Falzon O, Cassar K, Ellul C, Camilleri KP, Gauci J, et al. Establishing Differences in Thermographic Patterns between the Various Complications in Diabetic Foot Disease. Int J Endocrinol. 2018;2018:9808295. https://doi.org/10.1155/2018/9808295 17. Carabott M, Formosa C, Mizzi A, Papanas N, Gatt A. Thermographic Characteristics of the Diabetic Foot With Peripheral Arterial Disease Using the Angiosome Concept. Exp Clin Endocrinol Diabetes. 2021;129(2):93-8. https://doi.org/10.1055/a-0838-5209 18. Moreira DG, Costello JT, Brito CJ, Adamczyk JG, Ammer K, Bach AJE, et al. Thermographic imaging in sports and exercise medicine: A Delphi study and consensus statement on the measurement of human skin temperature. J Therm Biol. 2017;69:155-62. https://doi.org/10.1016/j.jtherbio.2017.07.006 19. van Doremalen RFM, van Netten JJ, van Baal JG, Vollenbroek-Hutten MMR, van der Heijden F. Infrared 3D Thermography for Inflammation Detection in Diabetic Foot Disease: A Proof of Concept. J Diabetes Sci Technol. 2020;14(1):46-54. https://doi.org/10.1177/1932296819854062 20. van Doremalen RFM, van Netten JJ, van Baal JG, Vollenbroek-Hutten MMR, van der Heijden F. Validation of low-cost smartphone-based thermal camera for diabetic foot assessment. Diabetes Res Clin Pract. 2019;149:132-9. https://doi.org/10.1016/j.diabres.2019.01.032 21. Kanazawa T, Nakagami G, Goto T, Noguchi H, Oe M, Miyagaki T, et al. Use of smartphone attached mobile thermography assessing subclinical inflammation: a pilot study. J Wound Care. 2016; 25(4):177-80, 182. https://doi.org/10.12968/jowc.2016.25.4.177 22. Fernández-Cuevas I. Aplicación de la termografía infrarroja para la prevención, seguimiento de lesiones y apoyo al diagnóstico en el deporte y la salud. En: 15º Congreso Internacional de Ciencias del Deporte y la Salud. [Zaragoza]: COLEFA; [2019]. p. 140-58. Available from: https://www.researchgate.net/profile/Ismael-Fernandez-Cuevas/publication/339816234_Aplicacion_de_la_termografia_ infrarroja_para_la_prevencion_seguimiento_de_lesiones_y_apoyo_al_diagnostico_en_el_deporte_y_la_salud/links/ 5e6755944585153fb3d1e1fa/Aplicacion-de-la-termografia-infrarroja-para-la-prevencion-seguimiento-de-lesiones-y- apoyo-al-diagnostico-en-el-deporte-y-la-salud.pdf [Accessed 2024 May 04] |
Enfermería Cuidándote. 2026; 9